The Troubled Teen Industry and Its Effects: An Oral History
{kind=link}
The troubled teen industry (TTI) is a term used to describe a system of underregulated residential youth treatment facilities that operate primarily in the United States. My research, which was funded by a 2021 Summer Undergraduate Research Fellowship (SURF) through the Hamel Center for Undergraduate Research, focused on gaining firsthand insight into the effects of one such treatment facility. These facilities, also referred to as treatment programs and treatment centers, constitute a multibillion-dollar industry and are infamous for numerous abuse charges (Stull, 2021). Adolescents are sent to these facilities for a myriad of reasons, ranging from severe mental health symptoms to more mundane forms of misbehavior (e.g., truancy). Parents are often manipulated through fear tactics into believing their children desperately need this type of facility, and are then manipulated to not believe their children if they say anything bad about the facility (Behar et al., 2007). Introduction to such facilities often includes involuntary youth transport, which consists of being woken up in the middle of the night by strangers; physical force is used if the adolescent does not comply (Stull, 2021).

The author, Jamie Mater.
Since its inception about 60 years ago, countless children have been processed through the TTI; current estimates in the United States are 120,000–200,000 children in the TTI at any given time (Krebs, 2021). The origins of the TTI can be traced back to the 1958 cult Synanon, a drug addiction rehabilitation center that used attack therapy, isolation, limited freedom, and rewards for compliance (Szalavitz, 2006). Since Synanon, an industry composed of wilderness therapy programs, boot camps, residential treatment centers, therapeutic boarding schools, religion-based programs, and drug rehabilitation programs has arisen (Lynch et al., 2016; Mohr, 2009).
The TTI came under significant scrutiny in 2006, with the publication of Maia Szalavitz’s Help at Any Cost, a book analyzing the industry (Stull, 2021). However, very little has been done to change the industry, and there is still a noted lack of regulations. Some facilities have been shut down, but many have rebranded and reopened. Survivors report physical abuse, exploitation (human trafficking), and several types of psychological torment, including harsh discrimination and LGBTQ+ conversion therapy. Multiple adolescents have even died in these facilities (Mohr, 2009). The treatment methods and their outcomes have not been properly studied and are often not supported by the best mental health practices.
I was a resident in TTI programs from the ages of 13 to 16. My longest stay was 18 months in a residential treatment center. Despite claiming no religious affiliation, the program’s model is based on a book of step-by-step skills significantly guided by Christian ideals. Residents’ behavior is reinforced through a point card system, which involves “earning” positive and negative points based on one’s behavior. Punishments are employed if a resident does not “earn” enough points. This program approach is an example of point-and-level systems used within the TTI. Because of my own experiences and a lack of in-depth research on these programs, I decided to study the experiences of former residents of a center of this type. My goal was to create an oral history that could be used to help foster an understanding of how TTI survivors have been affected and contribute knowledge that could lead to positive change in the TTI.
Methods
I gained approval for this project through the University of New Hampshire’s Institutional Review Board. Participants were recruited from two social media groups of people who had attended a specific treatment center in the southwestern United States. I created an anonymous account for the purpose of recruiting participants, and my intentions were made clear when I joined the groups. Through the anonymous account, I posted an outline of the project and invited people to be interviewed. Participants were offered a twenty-dollar gift card for their contribution.
I interviewed 19 adults, ages 19–26, who had been at this treatment center at some point in the last 10 years (largely between 2013 and 2017) and were sent there as minors. All participants were assigned female at birth, as according to the center’s entry criteria; however, five participants identified themselves as something other than a woman while in treatment or afterward. One participant had always identified as heterosexual, and two participants identified as heterosexual currently but did not while in treatment. Five participants identified themselves as people of color. One participant was not from the United States.
I conducted the interviews securely over Zoom, and participants gave verbal consent to be recorded. Participants were asked questions about their experiences before, during, and after treatment. (The complete interview questions appear in the Appendix.) I asked follow-up questions when necessary. After the questions had been answered, I thanked participants and provided them with a list of resources to help support them in the event of emotional distress. The Zoom transcription feature was used during the interviews for a baseline transcript, and I went through each interview afterward to edit the transcriptions for accuracy. Throughout the interviews, I noted topics that came up multiple times. The interviews were then coded using a grounded theory approach, in which I identified major themes and subthemes that consistently emerged within participants’ responses.
The following is a series of themes that surfaced from the interviews. This is a summarized version; the full results are being submitted to academic journals.
Summary of Past Experiences
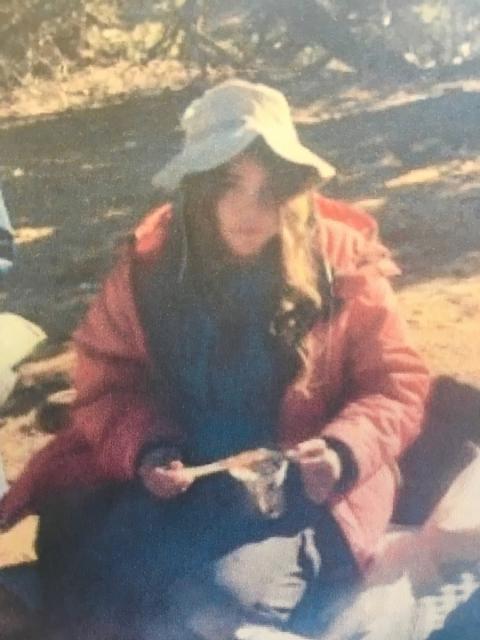
The author, age 13, eating with a stick in wilderness therapy. They were forced to do this every time they ate for three months.
Conflict with parents/guardians existed for most participants before treatment, ranging from problematic parenting techniques to extreme child abuse. All participants had experienced this and/or other forms of trauma. Participants faced a wide range of mental health issues before treatment, the most common being suicidality and depressive disorders. Other major issues included anxiety disorders, post-traumatic stress disorder, obsessive-compulsive disorder, dissociative disorders, neurodevelopmental disorders, and LGBTQ+-related issues. Most participants adopted harmful coping mechanisms, including self-harm, disordered eating, and substance use.
All participants had experienced some form of inpatient treatment prior to the facility focused on in this study, with most attending other programs and a few having been only in mental hospitals. Participants described entering treatment as a traumatic experience. One person who experienced involuntary youth transport remembered feeling “terrified” as they realized their parents had “hired kidnappers.” Another was “forced to undress” while a transporter watched. About half of participants were in other residential facilities before coming to the center at hand, with only one recalling a generally positive experience.
Over half of the participants had attended wilderness programs, and experiences varied from very negative (as recounted by most) to very positive (as recounted by a few). One person explained a common intake experience: “They made me strip completely naked and cough and squat in front of two staff. I’d never been naked in front of anyone. I was 14.” Other participants recounted being taught “self-hatred,” being “treated like animals,” and going “three weeks [without] wash[ing] our bodies” in the wilderness programs they attended. Positive experiences reported by participants were attributed to supportive staff and program philosophies encouraging self-love and acceptance. One person believed “wilderness saved [their] life.” However, even those with more positive experiences recalled witnessing harm inflicted by staff on peers, staff automatically distrusting them, and having their progress negated once they left.
Abuse and Neglect During Treatment
Throughout the interviews, I noted abuse by staff and therapists, as well as medical neglect. Many participants discussed daily instances of staff abusing power, with one explaining that “a system [like this] produces and reinforces evil behavior.” Multiple participants recalled being abused for having panic attacks, including being “sat on” and being “chased” by a staff member to the point of “hyperventilating in the grass just crying and panicking.” Many also recalled the program’s academic staff purposefully going against students’ needs.
Participants reported numerous inappropriate behaviors from therapists, including oversharing, forcing clients to be kind to abusive parents, victim-blaming, and ignoring some of clients’ major issues—or even telling them they were making up previous traumas. One therapy group at the center was for survivors of sexual trauma and was so poorly run that one participant believed the therapist should “[not] ever be allowed to talk to a survivor again.”
In addition, many participants reported problems with medications. Two participants mentioned a situation in which several people were prescribed the same medication for a number of unrelated issues, which did not help and caused health problems. One participant was prescribed incredibly high amounts of a medication, recalling that “the first psychiatrist [they] saw when [they] got out was shocked that [they] hadn’t died.”
Most participants had experiences of not being believed about health issues, which were life threatening in a few cases. One person was not allowed to speak without permission as part of their treatment, during which they got very sick, and said, “I was coughing up blood, and [the staff] wouldn’t let me talk so I could ask to go to the doctor.” They were not taken to a doctor until they were hours from developing a life-threatening infection.
Discrimination
Participants reported discrimination in many forms. Numerous participants felt they were dehumanized and “criminalized for having mental health issues.” Many participants had ADHD and/or autism, which was not acknowledged at the center. “A lot of the things they punished us for were just ways neurodivergent people try to relate to others,” explained one.
Multiple participants who identified themselves as a person of color also recalled experiencing discrimination. “I think I wasn’t taken as seriously academically; assumptions were made,” responded one participant. Another had previously experienced blatant racism in their wilderness program, as well as a few incidents while attending the program at hand, including an instance in which a peer made racist comments toward them and staff ignored it.
Numerous participants reported direct discrimination for their gender and/or sexuality. Several others recalled witnessing “many people get different rights taken away over their sexuality,” and hid their own sexualities to avoid discrimination. However, these same people “did experience consequences for engaging in what [was] deemed queer behavior.” Many participants recalled being scared to develop close friendships because of how staff might interpret it. Multiple people had staff members stop them from discussing sexuality, with one being told “you’re going to hell.”
Cult Tactics Used at the Facility
Before the Synanon cult was disbanded, other facilities were created using similar methodologies, for the purpose of profit. The TTI as it stands descends from Synanon and the other cults that were based on it (Szalavitz, 2006). Cult tactics used in the TTI include conversion therapy, linguistic control, coercive persuasion, and control over individuals’ bodies.
Multiple participants reported conversion therapy by name when describing the approach used at the facility. Several participants were told by their therapists that their female crushes were “grooming” them, and one was told that “if [they] were to get with a woman after treatment, it would be a sign of relapse.” Transgender people were forced to change their names and pronouns, and their peers were punished for using the ones they preferred. One person shared that questioning their gender was “listed on [their] reasons for admission” and that they left “a lot more feminine.” Participants also reported that “self-care was conflated with femininity.”
Linguistic control was evident in several forms at the facility. Participants noted that they could not speak about certain topics (e.g., sexuality, politics, and traumatic incidents that occurred within the center), had to follow specific “unnatural” rules when speaking, could only speak positively about the center, could not speak to strangers in public, and were monitored any time they spoke. Regular punishments restricted permission to speak, occasionally for months-long periods. One participant kept a personal journal in a foreign language and “found Google translations of it in the home manager’s office.” Throughout the interviews, all participants but one used treatment-specific terms that could only be understood by people who had been in the TTI themselves, meaning that their speech is still impacted by their time in the TTI.
Reports of extreme manipulation were common. In almost every interview, participants described “a full, complete loss of any self-identity.” As one person explained, “They have a very specific model of girl that they want you to be, and that’s how you progress.” Numerous participants “became submissive,” and some believed that “following everything they said” was the only way to succeed in life. Many underwent “public humiliation and shaming” from their peers for noncompliance. Participants who tried to tell their parents what was happening were not believed. The point system was called “suppressive” and “controlling” and punished participants for showing emotion. Those who turned 18 at the center were legally allowed to leave, but could not take their phone, ID, money, or medications.
Participants’ bodies were controlled in many ways, with one expressing that they “felt like [they] didn’t have any autonomy.” Participants were “made fun of” by staff when they tried to state their rights. Many mentioned being forced to clean “to an extreme.” Participants were also punished for having nightmares, forced to sleep on the floor, and not allowed platonic physical touch, and had to cut their hair and dress in approved ways. They were taught “disordered eating habits,” including being forced to eat foods they found disgusting, having to eat exact serving sizes (and sneaking food due to hunger), being rewarded with unhealthy foods, and having food options restricted as punishment. One person was “forced to eat meat a lot” despite trying to be a vegetarian.
Exacerbation of Symptoms During Treatment
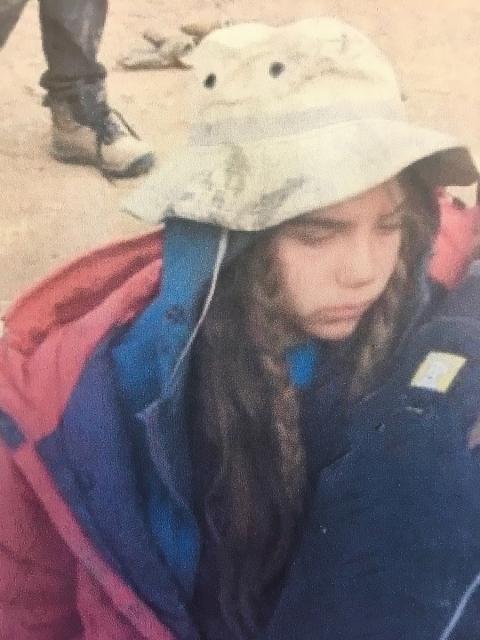
Candid photo of the author, age 13, sitting in a catatonic state while in the TTI.
Participants noted that the distress they felt before treatment was only worsened by the program. While in the program, participants mainly felt “anxious,” “stressed,” “lonely,” “hopeless,” and “trapped.” One participant recalled, “I was always on edge, thinking, ‘What am I doing wrong right now?’” Another “felt empty, like an experiment or a puppet.” Overall, participants’ “emotional needs weren’t being met.” Most coped with difficult times by dissociating, because “it was better than feeling the reality of being there.” A few cried often, but “silently.” Participants also returned to or learned behaviors such as self-harm and disordered eating. Those who wanted to use healthy coping mechanisms stopped depending on them, because “they got taken away so easily” or were not available in the first place.
Almost every participant’s positive memories of the program were of friendships and/or animal-assisted therapy. When asked about negative memories, there were often comments of “there’s a lot of those.” Responses typically involved general distress or specific traumas. These traumas included peers harming themselves or participants and staff abusing participants or their peers.
Transition to Life After Treatment
Participants reported a variety of difficulties after leaving treatment. Some mentioned trouble “assimilating back into society,” due to it being so different. Many reported variations of “having to be constantly reminded that [they] did not need to ask for permission to do everything,” and not being able to relax because they had been conditioned by the program to do chores constantly.
Some participants struggled soon after their release, while others experienced a brief period of believing they were mentally healthy, followed by a crash. Several were admitted to mental hospitals within a year. Some “felt deprived of normal experiences” and began engaging in risky behaviors. Relapsing into old problems was very common, as was developing new issues as a result of treatment; eating disorders commonly emerged.
Many participants reported that they currently experienced symptoms of post-traumatic stress disorder (PTSD), such as nightmares, panic attacks, dissociation, memory issues, flashbacks, and hypervigilance. Multiple participants reported experiencing PTSD by name. Participants were triggered by small daily things, such as “grocery stores, cooking, and cleaning,” and experienced stress if they did not follow the program’s rules. “I feel like I live in two worlds,” expressed one. Many wanted to seek professional help but could not due to fear of therapists and medications. People often still struggled with the same issues they were sent to treatment for and had difficulties with school and/or work. Many had ongoing identity issues, and often still felt “ashamed” over their sexuality and/or gender.
Participants reported feeling “angry,” “utterly hollow,” and “like [they’re] drowning” when thinking about their time in the program. Most thought about their time in treatment multiple times a week, some as often as “a couple times an hour.” Some had avoided thinking about it for years until recently. Most participants said the program had a negative impact on their lives, with a few viewing it as a bad experience that drove them to a more successful place. No participant would recommend this center to a struggling teen, and distress was common about children still being there.
Influences on Relationships
Participants expressed that family relationships were strained after treatment, mainly because of family members not understanding what participants had gone through and not putting in genuine effort to become healthier people themselves. Some became closer with their families in “superficial” ways, and those who had good relationships beforehand “lost that connection.” Previously harmful home environments remained harmful, and several participants’ parents threatened to send them away again.
Many participants “had no friends” when they came back, as a result of being gone for so long and being ostracized for disappearing. Making new friends was very difficult, because of not knowing “how to interact with people,” not being “able to talk about the past,” and peers having “[built their] identities on the last couple years, because they were very formative years.” A few participants currently only had close friends from treatment, despite having been out for many years. People also struggled with assertiveness in romantic relationships, leading to abusive situations. Two relationship benefits arose: one participant’s parent put in hard work to be healthier, and participants who are now parents are dedicated to raising their children well.
The social media hashtag #breakingcodesilence has been used by thousands of TTI survivors to discuss their experiences online. TTI advocacy groups include Unsilenced (unsilenced.org), the We Warned Them campaign (wewarnedthem.org), and Breaking Code Silence (breakingcodesilence.org).
Methods of Healing
Although participants were still struggling in many ways at the time of the interviews, they had also found healthy ways to move forward with their lives. For some, this meant moving away from harmful home environments. For LGBTQ+ participants, it was “really healing” to embrace their identities, including transgender individuals transitioning. Outside influences helped as well, such as apologies from staff and knowledge of related activism. The biggest help, regardless of life situation, was getting genuinely good therapeutic assistance and/or (re)connecting with others who had been through treatment: “I felt like I was going insane until I connected with someone else from treatment, and they were like, ‘No, those are real memories.’”
Conclusion
Readers unfamiliar with this subject may be surprised that treatment centers such as this one still operate with few repercussions. Those familiar with this subject who were not clients themselves may be surprised to see these centers portrayed like this, as they advertise themselves as ideal facilities with pure intentions and proper techniques. The research I completed is a much-needed analysis of the harsh realities behind centers such as this one. With a history rooted in cults and a focus on behavioral change instead of genuine growth, it is hard to find any good within the TTI. It would be very difficult to reform it into anything helpful. However, that does not mean that certain regulations should not be put in place as soon as possible to reduce harm.
This research project was the hardest thing I have ever done, but it was incredibly therapeutic as well. Living with this trauma has been very difficult, and systematically analyzing it as a collective trauma required me to find strength and love I didn’t know I had. After feeling helpless for a long time, I took it upon myself to do something about this issue, and I can only hope that I have successfully conveyed the truth of what we and countless others continue to go through.
I would like to thank my mentor, Dr. Robert Eckstein, for his support and guidance throughout the process of this research. I would also like to thank the Hamel Center for Undergraduate Research and the Rogers Family Undergraduate Research Fund, established by the Rogers Family Foundation, Dana Hamel, and Kristen Butterfield-Ferrell, for providing financial support for my Summer Undergraduate Research Fellowship and helping to make this project possible. Next, I would like to thank all of the participants in this research, as this is not an easy subject to talk about. Lastly, I would like to thank my friends and fellow TTI survivors Sam Doe and Tashi McKellop for their ongoing support and feedback since the beginning of this project.
References
Behar, L., Friedman, R., Pinto, A., Katz-Leavy, J., & Jones, H. W. (2007). Protecting youth placed in unlicensed, unregulated residential “treatment” facilities. Family Court Review, 45(3). https://doi.org/10.1111/j.1744-1617.2007.00155.x
Krebs, C. (2021, October 22). Five facts about the troubled teen industry. Americanbar.org. Retrieved February 26, 2022, from https://www.americanbar.org/groups/litigation/committees/childrens-rights/practice/2021/5-facts-about-the-troubled-teen-industry/#:~:text=Descriptions%20of%20experiences%20in%20the,needs%20like%20food%20and%20water.
Lynch, S. E., Teich, J. L., & Smith, K. E. (2016). Psychiatric residential treatment centers for children and adolescents: Modeling variation in Facility Definition Type. Journal of Child and Family Studies, 26(4). doi:10.1007/s10826-016-0640-1
Mohr, W. K. (2009). Still shackled in the land of liberty. Advances in Nursing Science, 32(2). doi:10.1097/ans.0b013e3181a3b16f
Stull, O. A. (2021). An exploratory study on adult survivors of the troubled teen industry’s therapeutic boarding schools and wilderness programs. Publication No. 28027111. [Doctoral dissertation, University of Kansas]. ProQuest Dissertations Publishing.
Szalavitz, M. (2006). Help at any cost: How the troubled-teen industry cons parents and hurts kids. Riverhead Books.
Author and Mentor Bios
Los Angeles native Jamie Mater will graduate in spring 2022 with a bachelor of arts in psychology and a minor in linguistics. Their research, which was funded by a 2021 Summer Undergraduate Research Fellowship (SURF) through the Hamel Center for Undergraduate Research, was driven by their passion and experiences surrounding the troubled teen industry. For Jamie, this was more than just a research project; it was a way of confronting the pain of their own experiences in a healthy way, while also shedding light on all the issues within the troubled teen industry. Through their interviews, Jamie was able to create a space where survivors could share their stories and Jamie could document the collective feelings and experiences they all still carry with them to this day. This research was the first step in a larger body of research that Jamie hopes to do after getting their PhD. Jamie hopes to identify problems within mental health treatment and to find more effective ways of addressing mental health issues.
Robert Eckstein is a senior lecturer in psychology and justice studies who started teaching at the University of New Hampshire in 2004. The majority of his research and consultations is centered around gender-based violence. Although Dr. Eckstein has mentored many undergraduate research students, Jamie is his first mentee to publish their work in Inquiry. One of the reasons Dr. Eckstein loves teaching is the opportunity it gives him to work with students who are passionate and enthusiastic about what they are learning, and he saw this in Jamie while working on their project. He shared that his experience working with Jamie was very satisfactory. Dr. Eckstein believes that Inquiry gives students an important opportunity not only to share their impressive research, but develop valuable skills in different styles of writing.
Copyright 2022, C. Jamie Mater